The treatment of trauma with topographic guided ablation is dependent on the level of scarring caused by the trauma, the position of the scarring, and the amount of corneal tissue available for correction. All repair cases must be evaluated individually, and trauma cases even more so as the extent and depth of corneal scarring must be determined to see if improvement can be made. We have treated scissors going through cornea, animal claw caused corneal ruptures, skateboarding accident corneal damage, flying metal damage, and others.
Infection repair can be similar to trauma repair, as it depends on the level and position of scarring, and how much tissue was lost due to the infection. Again, this must be evaluated individually for each patient. We have treated a variety of infection caused corneal damage.
Critical is the amount of tissue available, and the depth of the scarring. Even scars that are determined to be “full thickness” by doctors many times are not, and improvement can be achieved by removing enough tissue to allow for vision while leaving enough for structural integrity.
The CREATE Protocol here is still useful, as many of these cases do have significant epithelial compensation and must be treated with regard to this. In many way, these patient require a more individualized approach in comparison to other repairs
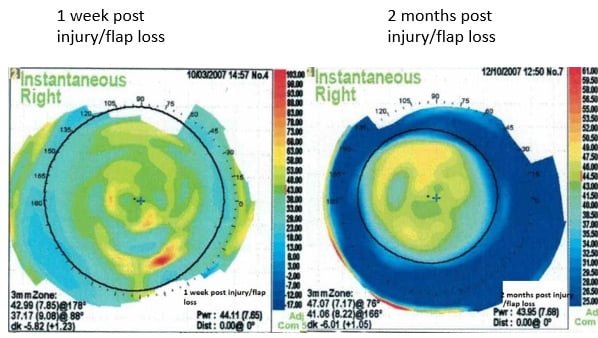
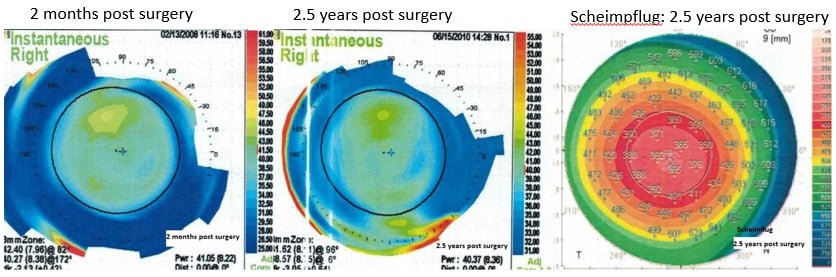
The second case on this page was a traumatic flap loss of a prior LASIK, and correction of this was performed before topographic guided ablation was available, so normal aspheric ablation laser correction was performed. It is included here as an interesting case to show that even flap loss does not mean that a patient cannot have a good outcome of their vision.
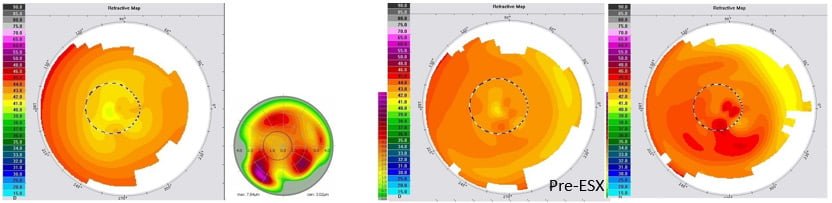
46 year old male, OD T-CAT + WFO PRK.
Pre-Op Manifest; OD: +3.25-0.25X010 BCVA 20/40
T-CAT Treatment; OD: +0.00-0.25X054
WFO Treatment; OD: +1.00 D/S
1 ENH WFO; OD: +2.25 D/S
1 Year Post Op: OD Refraction: +1.00 and 20/25
35 year old male, OD LASIK
Pre-Op Manifest; OD: -5.25-0.50X180 BCVA: 20/20
Pre-Op Pachymetry; OD: 560
PRK ENH 4 years later; OD: -5.00-1.25×090
Post Injury Pachymetry; OD: 462
2.5 year Post-Op; plano and 20/15

Cataract Surgery is the most performed surgical procedure in the United States, and has a phenomenal track record for improving…
Read More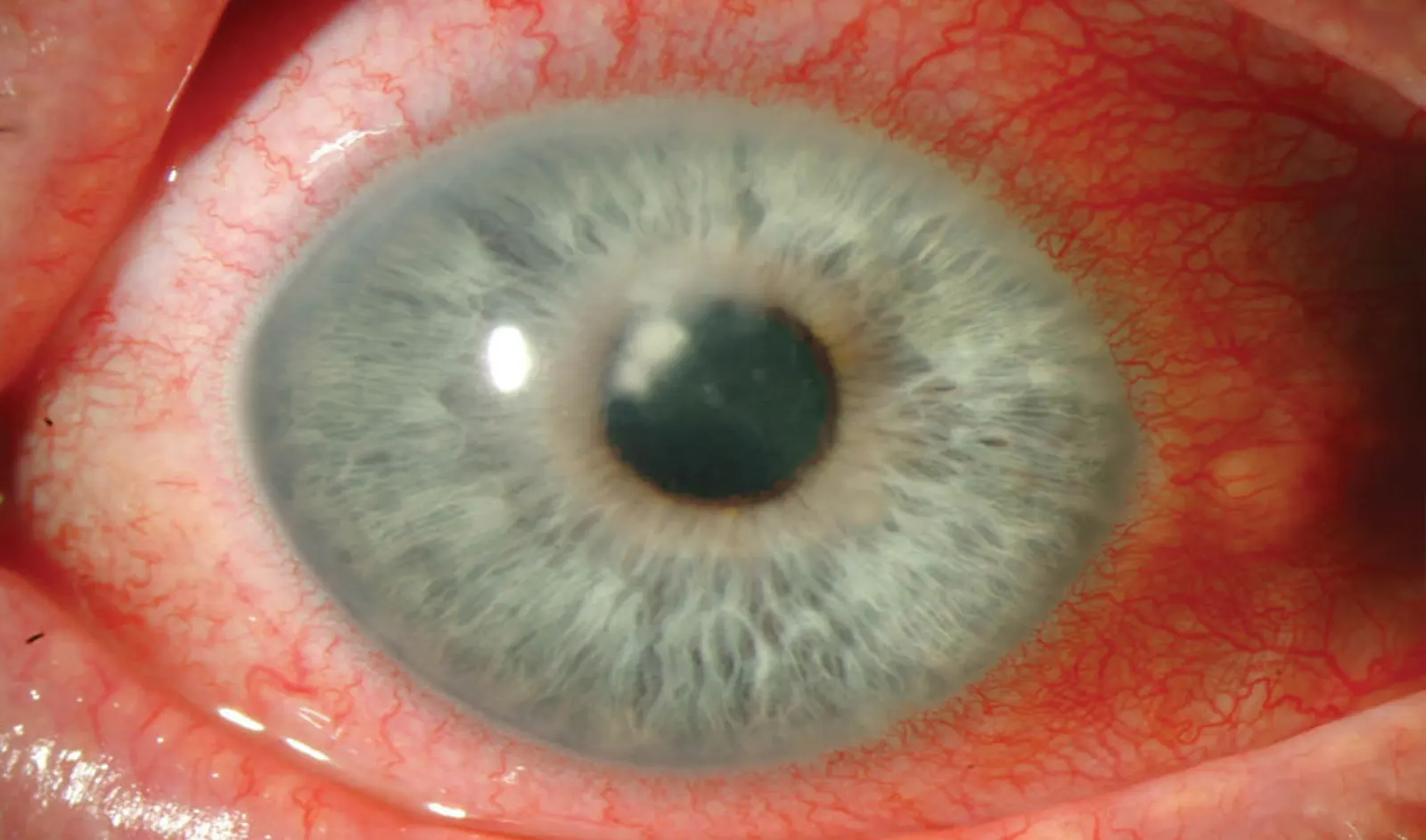
The treatment of trauma with topographic-guided ablation depends on the level of scarring caused by the trauma, the position of…
Read More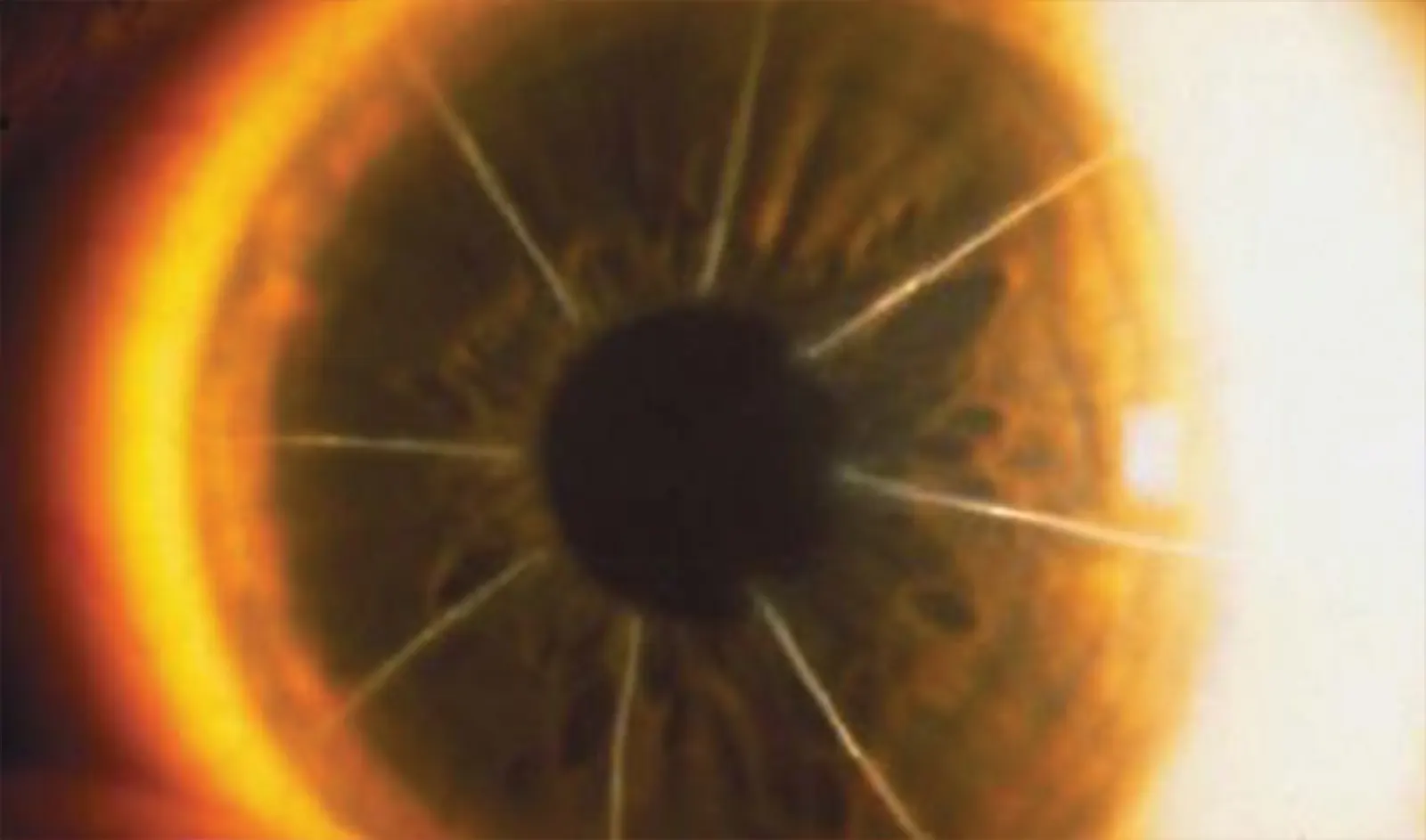
In the dynamic world of eye care, keratoconus treatment has become a focal point due to the condition’s impact on…
Read More